Muscle imbalances are quite common in people, even world-class athletes. The muscles on the front of the thigh (quadriceps) are quite often stronger than the muscles on the back of the thigh. And the upper trapezius muscles tend to be stronger than the lower trapezius muscles. The anterior deltoids are stronger than the posterior deltoids. As a rule, they develop the muscles that a person sees and they are located in front. The shoulder is a classic example of a body part that people try to develop first. It's no surprise that 30% of all strength training injuries occur in the shoulder joint.
The shoulder muscles can be divided into two groups:
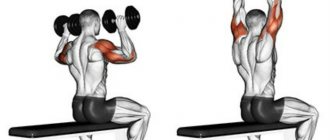
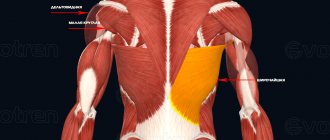
- Flexors and extensors and these include the deltoid muscle, supraspinatus and infraspinatus muscles, teres minor and major muscles, subscapularis muscle. The deltoid muscle has the most complex and diverse functions. The deltoid muscle consists of three bundles
- The anterior deltoid muscle is located in the front of the shoulder, the lateral deltoid muscle is located in the middle of the shoulder, and the posterior deltoid muscle is located in the back of the shoulder.
Data from a study of bodybuilders showed that the strength of the anterior deltoid muscle could be 5 times greater than that of ordinary people. And the lateral deltoid muscles could be 3 times stronger. At the same time, oddly enough, the rear deltoid muscles were only 15% stronger.
The muscle imbalance between the front and rear deltoids can be partly explained by the emphasis on exercises that target the front deltoids and the lack of exercises that target the rear deltoids.
Coordinated work of the shoulder muscles allows you to perform the necessary movements and maintain stability of the shoulder joint. A disruption in the interaction of the muscles that stabilize the shoulder with the muscles that perform movements is called a muscle imbalance of the shoulder. This disorder creates problems with movement, since the muscles responsible for movement are stronger than the muscles responsible for stability and this leads to instability.
In most cases, muscle imbalance can occur due to repetitive movements. The most common is excessive strengthening of the internal rotator muscles of the shoulder accompanied by poor development of the external rotator muscles. The internal rotator muscles are strengthened with chest exercises and back exercises, but the external rotator muscles are rarely worked. This leads to rotator cuff imbalance and damage to both the rotator cuff muscles and tendons. This imbalance can be corrected with specific exercises to strengthen the external rotation muscles.
Content
- 1 Deltoid muscle, clavicular part 1.1 Beginning
- 1.2 Attachment
- 1.3 Innervation
- 1.4 Training
- 1.5 Features
- 1.6 Shoulder flexion/adduction. Functional muscle tests
- 1.7 Participation in sports
- 2.1 Beginning
- 3.1 Beginning
Clinical significance[edit]
The most common abnormalities affecting the deltoid muscle are tears, fatty atrophy, and enthesopathy. Deltoid tears are uncommon and are often associated with traumatic shoulder dislocation or massive rotator cuff tears. Muscle wasting results from a variety of causes, including aging, disuse, denervation, muscular dystrophy, cachexia, and iatrogenic injury. Deltoid enthesopathy of the humerus is an extremely rare condition associated with mechanical stress. Conversely, deltoid acromial enthesopathy is likely to be a feature of seronegative spondyloarthropathies, and its detection should probably be accompanied by appropriate clinical and serologic testing. [24]
Deltoid muscle, acromial part[edit | edit code]
Deltoid muscle, acromial part
Home[edit | edit code]
- Akromion
Attachment[edit | edit code]
- Deltoid tuberosity of the humerus
Innervation[edit | edit code]
- Axillary nerve, C5-C6
Features[edit | edit code]
The acromial part of the deltoid muscle (m. deltoideus) forms the relief of the lateral part of the shoulder girdle. When lifting heavy objects, it holds the head of the humerus in the glenoid cavity of the scapula.
| Functions | Synergists | Antagonists |
| Shoulder abduction (with the arm already abducted) | *M. deitoideus (spinous and clavicular parts with the arm already abducted) *M. infraspinatus (cranial part) *M. biceps brachii (long head) | *M. pectoralis major *M. latissimus dorsi *M. teres major *M. teres minor *M. coracobrachialis *M. biceps brachii (short head) *M. deitoideus (clavicular and spinous parts with the arm already adducted) *M. infraspinatus (caudal part) *M. triceps brachii (long head with arm already abducted) |
Shoulder abduction. Functional muscle tests[edit | edit code]
Issues and comments
- Do not allow the patient to externally rotate the arm, as this will engage the biceps brachii muscle.
- When testing the acromial deltoid, ensure that the patient does not elevate the shoulder or tilt to the opposite side, as this may appear to be shoulder abduction.
- The supraspinatus muscle serves as an assistant to the acromial part of the deltoid muscle.
Participation in sports[edit | edit code]
The acromial part of the deltoid muscle is involved in all sports that require abduction of the upper limb from the starting position (fencing, weightlifting) or holding the shoulder in an abducted position (archery, rifle shooting). This muscle plays an important role in all types of swimming, especially crawl and butterfly. When doing weightlifting, it centers the head of the humerus in the glenoid cavity of the scapula.
| Kind of sport | Movement/hold | Function | Load | Types of abbreviations |
| Fencing | Lunge | Shoulder abduction | Fast, explosive | Dynamic concentric |
| Weightlifting | Thrust phase | Shoulder abduction | Fast, explosive, maximum | Dynamic concentric |
| Handball | Throw | Shoulder stabilization | Fast | Dynamic concentric |
| Thrust phase | Stabilization of the humeral head in the glenoid cavity | Fast | Dynamic concentric | |
| Archery | Bowstring tension and aiming | Stabilization of the upper limb in abduction position | Strength endurance | Static |
| Rifle shooting | Stabilization of the upper limb in the shooting position | Stabilization of the upper limb in abduction position | Strength endurance | Static |
| Swimming | Breaststroke, backstroke - carry phase | Shoulder flexion, shoulder abduction | Strength endurance | Dynamic concentric |
| Swimming crawl or butterfly - carry phase | Shoulder abduction | Strength endurance | Dynamic concentric |
Other animals[edit]
The deltoid muscle is also found not in humans, but in members of the great ape family. The human deltoid muscle is the same proportional size as the rotator cuff muscles in monkeys such as the orangutan, which are involved in the shoulder joint and have the muscle mass needed to support the body's weight with the shoulders. In other apes, such as the common chimpanzee, the deltoid muscle is much larger than in humans, weighing on average 383.3 grams compared to 191.9 grams in humans. This reflects the need to strengthen the shoulders, especially the rotator cuff, in joint-walking monkeys to support whole body weight. [2]
The deltoid muscle is a major component of the wing musculature of bats and pterosaurs [25], but is greatly reduced in crown group birds because they have a preference for muscles attached to the sternum. However, some Mesozoic flying theropods had more developed deltoid muscles. [26]
Read also[edit | edit code]
- Muscles - anatomy and functions
- Muscles of the shoulder girdle
- Arm muscles
- Shoulders - exercises and training features
- Anatomy of the shoulder joint
- Trapezius muscle
- Levator scapulae muscle
- Rhomboid muscles
- Serratus anterior muscle
- Supraspinatus muscle
- Infraspinatus muscle
- Subscapularis muscle
- Latissimus dorsi muscle
- Teres major muscle
- Teres minor muscle
- Pectoralis major muscle
- Pectoralis minor muscle
- Subclavius muscle
- Coracobrachialis muscle
Links[edit]
- Brown, J.M.; Wickham, J.B.; McAndrew, DJ; Huang, X. F. (2007). "Muscles within Muscles: Coordination of 19 muscle segments in three shoulder muscles during isometric movement tasks." J Electromyogr Kinesiol
.
17
(1):57–73. DOI: 10.1016/j.jelekin.2005.10.007. PMID 16458022. - ^ a b c d
Potau, J.M.;
Bardina, X; Ciurana, N; Camprubi, D. Pastor J.F.; de Paz, F. Barbosa M. (2009). "Quantitative analysis of the deltoid and rotator cuff muscles in humans and great apes." Int J Primatol
.
30
: 697–708. DOI: 10.1007/s10764-009-9368-8. - Anatomy of the Shoulder Muscles: “The deltoid is the triceps muscle that covers the shoulder. The three heads of the deltoid muscle are anterior, intermediate and posterior."
- ^ a b c
"Deltoid muscle". Wheeless "Textbook of Orthopedics. December 2011. Retrieved January 2012. Check date values in: |access-date=(help) - Leijnse, JNAL; Khan, S.H.; Kwon, Y. H. (December 2008). "Morphology of the deltoid and terminal tendons - a universal model". J Anat
.
213
(6):733–742. DOI: 10.1111/j.1469-7580.2008.01000.x. PMC 2666142. PMID 19094189. - Anterior deltoid
- ^ a b
Take your delts from Muscle and Fitness: "target point: front/middle delts" - ^ a b
Lateral deltoid - Best Exercise for Outer Delts on LiveStrong.com in 2011
- Shoulders Anatomy archived 04/28/2012 on the Wayback Machine by Yu Yevon
- Posterior deltoid
- Rear deltoid stretch
- Lee Hayward - Rear Delts
- Fick, R. (1911). Handbuch der Anatomie und Mekanik der Gelenke
. Jena: Gustav Fischer. - ^ a b
Kapandji, Ibrahim Adalbert (1982).
Physiology of joints: upper limb volume one
(5th ed.). New York: Churchill Livingston. - Sakoma, Yoshimasa; Sano, Hirotaka; Shinozaki, Nobuhisa; Itoigawa, Yoshiaki; Yamamoto, Nobuyuki; Ozaki, Toshifumi; Itoi, Eiji (2011). "Anatomical and functional segments of the deltoid muscle". Journal of Anatomy
.
218
: 185–190. DOI: 10.1111/j.1469-7580.2010.01325.x. PMC 3042752. PMID 21118198. - Rispoli, Damian M.; Athwal, George S.; Sperling, John W.; Cofield, Robert H. (2009). "Anatomy of the deltoid insertion" (PDF). J Shoulder Elbow Surg
.
18
(3):386–390. DOI: 10.1016/j.jse.2008.10.012. PMID 19186076. Archived from the original (PDF) on 09/04/2012. - Anatomy photo: 03:03-0103 at SUNI Downstate Medical. Kenhub
. Retrieved September 21, 2022. - ^ a b
Brown, JMM;
Wickham, J.B.; McAndrew, DJ; Huang, X. F. (2007). "Muscles within Muscles: Coordination of 19 muscle segments in three shoulder muscles during isometric movement tasks." Journal of Electromyography and Kinesiology
.
17
(1):57–73. DOI: 10.1016/j.jelekin.2005.10.007. PMID 16458022. - Avis, Duncan; Power, Dominic (2018-03-26). "Axillary nerve injury associated with shoulder dislocation". EFORT Open Reviews
.
3
(3): 70–77. DOI: 10.1302/2058-5241.3.170003. ISSN 2058-5241. PMC 5890131. PMID 29657847. - Upper limb radiography: 24 ARRT category A. CE4RT, 2014. 201. Print.
- "Archival copy". Archived from the original on 2012-06-25. Retrieved 17 June 2013.CS1 maint: archived copy as title (link)
- Rent CF. Ultrasound of the shoulder. Master Medical Books, 2013. Chapter on deltoid enthesopathy available at ShoulderUS.com.
- Witton, Mark (2013). Pterosaurs: natural history, evolution, anatomy. Princeton University Press. ISBN 978-0691150611.
- Voeten, Dennis FAE; and others. (2018). " (March 13, 2022). "Wing bone geometry suggests active flight of Archeopteryx". Nature Communications
.
9
: 923. DOI: 10.1038/s41467-018-03296-8. PMC 5849612. PMID 29535376.
The structure of the ulna
We have already understood that in the forearm there are two long tubular bones connected on both sides by joints. The third side of the ulna is called the medial side and faces inward, like its edges.
The ulna is located on the outside of the arm, which is called the medial position. For example, if we consider a limb on the left and right, the left forearm contains the ulna on the left and the right on the right. In other words, the ulna is located in the forearm on the little finger side.
The superior epiphysis of the ulna is thicker than the proximal epiphysis of the radius and articulates with it through a block-shaped depression, which is limited by two processes: the coronary and ulnar. On the inner side of the coronoid process there is a radial notch intended for the radial capital. The joint, together with the articular surface and cartilage, forms the elbow joint, which allows flexion and extension of the forearm.
The lower epiphysis, on the contrary, is thinner than the distal epiphysis of the radius and is connected to it using an articular circumference, and then passes into the wrist joint.
The structure of the radius
If the ulna is located medially, the radial third is not adducted: it is located on the inside of the arm, that is, located distally. For example, the left forearm (where the ulna is on the left) contains a radius on the right. In other words, the radius is on the thumb side.
The third side of the beam is called the side, it faces outward. The superior epiphysis consists of a head with a small depression in the center for connection with the condyle of the humerus. The distal pineal gland externally contains the ulnar notch for connection with the head of the ulna.
Fractures of the forearm bones
The bones of the forearm are quite thin, so they break easily even with minor injuries.
Forearm fractures can be divided into several types:
- Fracture of the elbow joint - occurs due to a fall on the elbow or due to a strong contraction of the triceps. It is characterized by swelling with a bluish tint, sharp pain when moving, deformation or drooping of the arm.
- Damage to the coronoid process - occurs due to a fall on a bent elbow. Complaints of swelling, limited movement and pain.
- Fracture of the proximal bone - caused by a fall on the elbow in a bent position.
- Fracture of the ulna or radius - occurs due to a direct blow. The main symptoms are swelling, severe pain and limited mobility.
- Fracture of both bones of the forearm - characterized by displacement of the broken bones and their convergence.
In case of fractures, it is extremely important to provide first aid to the victim. If the fracture is open, you should not try to fix it yourself. It must be remembered that two joints are necessarily immobilized: the wrist and the elbow. To do this, you can apply a splint without touching the side of the arm from which the bone protrudes.
The forearm is an important segment of the upper limb, providing high mobility of the hand and a variety of actions performed.
Connection of the bones of the forearm
An important role in the anatomy of the tubular bones of the forearm is played by the way they are connected to each other. The joints allow the radius to move around the ulna. The bone can move inward or outward, with the wrist and elbow joints always working together.
When moving, the radius describes an arc of 140 degrees to the ulna. In this case, the arm and shoulder are adducted, albeit with minor movement, for a total of 220 to 360 degrees of range of motion. It is the possibility of such rotation that allows a person to perform various movements with the upper limbs.
An important place in the connection of the bones of the forearm is occupied by the interosseous membrane, consisting of collagen fibers. It lies between the radial and ulnar crests and holds them in such a way as not to restrict movement.
Week schedule
The table below shows a weekly training schedule for the balanced development of all 3 deltoid muscle bundles.
| Day of the week | List of exercises for a specific day of the week |
| Monday | 1. Dumbbell press from a standing position. 2. Barbell press from the upper chest from a standing position. 3. Handstand push-ups upside down. 4. Lifting the body from the floor using your fists. |
| Tuesday | A day of rest and restoration of the muscular system. |
| Wednesday | 1. Pull-ups of dumbbells while lying on an inclined bench. 2. Lifting the barbell to the chin. 3. Raising dumbbells in different directions with their simultaneous rotation. 4. Dumbbell push-ups. |
| Thursday | The day of restoring the deltoid muscles, receiving high-quality and balanced nutrition. |
| Friday | 1. Side plank with forearm access. 2. Raising dumbbells in different directions from a sitting position in an inclined position. 3. Reverse butterfly with expander. 4. Bending your arm back. 5. Throwing the barbell in front of you. |
| Saturday | A day of rest and restoration of the muscles of the musculoskeletal system. |
| Sunday | Carrying out cardiological training to prevent cardiovascular diseases that can arise as a result of intense physical activity on the body using sports equipment. Sunday cardio training involves doing the following:
Walking outdoors can also be a great cardio workout option. |
Skipping a workout, drinking alcohol, and smoking do not have a positive effect on the development of deltoids. Excessive physical activity also has a negative effect on the formation of muscle tissue in the shoulder girdle.
Nerves of the forearm
The forearm, where many muscles are located, is also where nerves pass. Let's take a look at the main nerves located in this area and their functions:
- Median: branches are located in the elbow joint and the anterior muscles of the forearm. It innervates the joints of the hand and the muscles of the thumb.
- Medial cutaneous - innervates the skin of the forearm, originating from the medial bundle.
- Musculocutaneous - its branches are located in the elbow joint, descending below it in the form of the lateral cutaneous nerve. Innervates the skin of the forearm.
- Radial: The deep branch of this nerve innervates the extensor muscles of the forearm.
- Ulnar - located near the ulnar artery, innervates the flexor carpi ulnaris. Below it is divided into branches that innervate the palm from the inside and outside.